
Hypocalcaemia in children
Serum Calcium <1.1mmol/L
Causes
– Low stores in Prematurity, maternal diabetes or pre-eclampsia, high-phosphate containing milk
– Nutritional rickets or Vit D resistance
– Hypoparathyroidism (e.g. DiGeorge synd) or pseudohypoparathyroidism
– Drugs- Phenytoin, Cisplatin
Other- Alkalosis, Renal tubular acidosis, hypomagnesemia, acute pancreatitis
Clinical presentation
Chronic hypocalcaemia may be asymptomatic. Look for evidence of rickets, although hypocalcaemia is not always seen in vit D deficiency.
Neonates may present with poor feeding, vomiting, lethargy, jitteriness or seizures.
Children can manifest with carpopedal spasms, muscle spasms, tetany, paresthesias or seizures. Rarely laryngospasm or raised ICP.
Chvostek sign= tapping on cheek anterior to the external auditory meatuscauses twitching of the orbicularis oculi and mouth
Trousseau sign= inflating BP cuff above systolic pressure for 3min causes carpopedal spasm
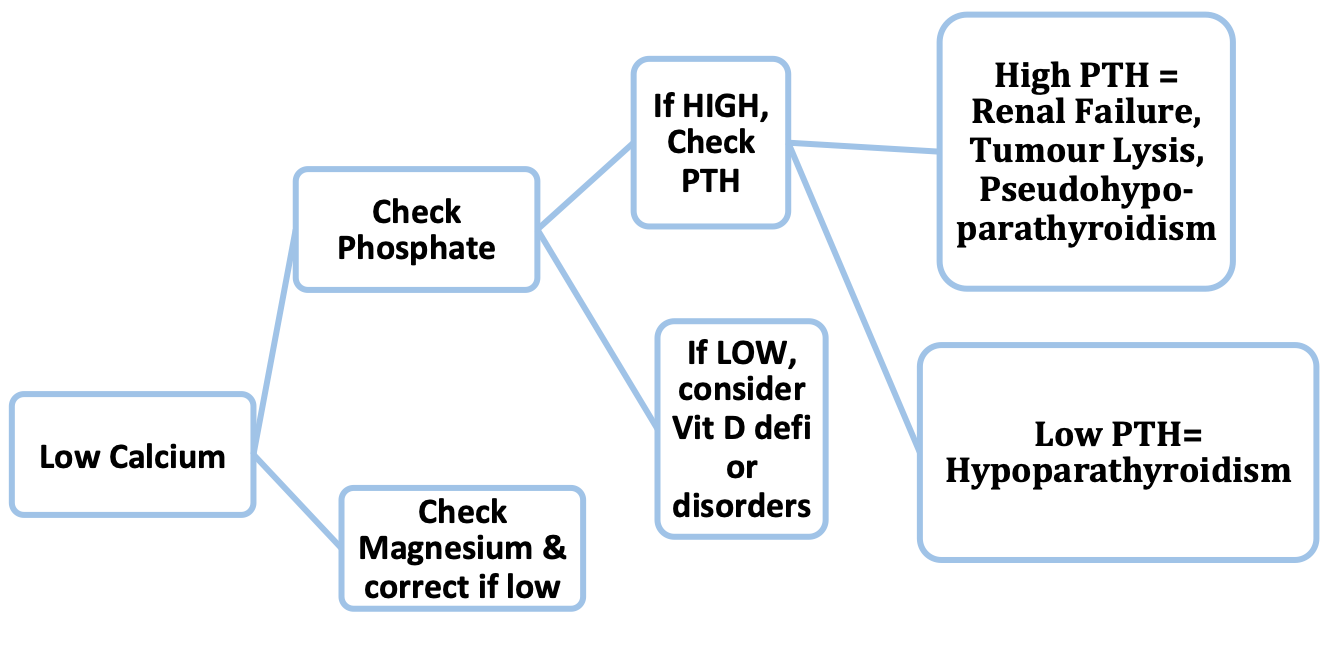
Investigations
– Recheck Serum Calcium & ionized Calcium with Albumin
– Also check Phosphate, Magnesium, Alk Phos, PTH and Vit D are initial tests
– ECG may show prolonged QTc, AV block and rarely VT
Management
Acute symptoms are treated promptly with IV Calcium Gluconate given under cardiac monitoring (extravasation may cause tissue necrosis).
This may be repeated every 6 – 8 hours initially.
If asymptomatic, commence oral Calcium supplement and monitor bone profile.
If low Vit-D, give Cholecalceferol or Calcitriol
If low Magnesium, give IV MgSO4 as hypocalcemia may be otherwise refractory