
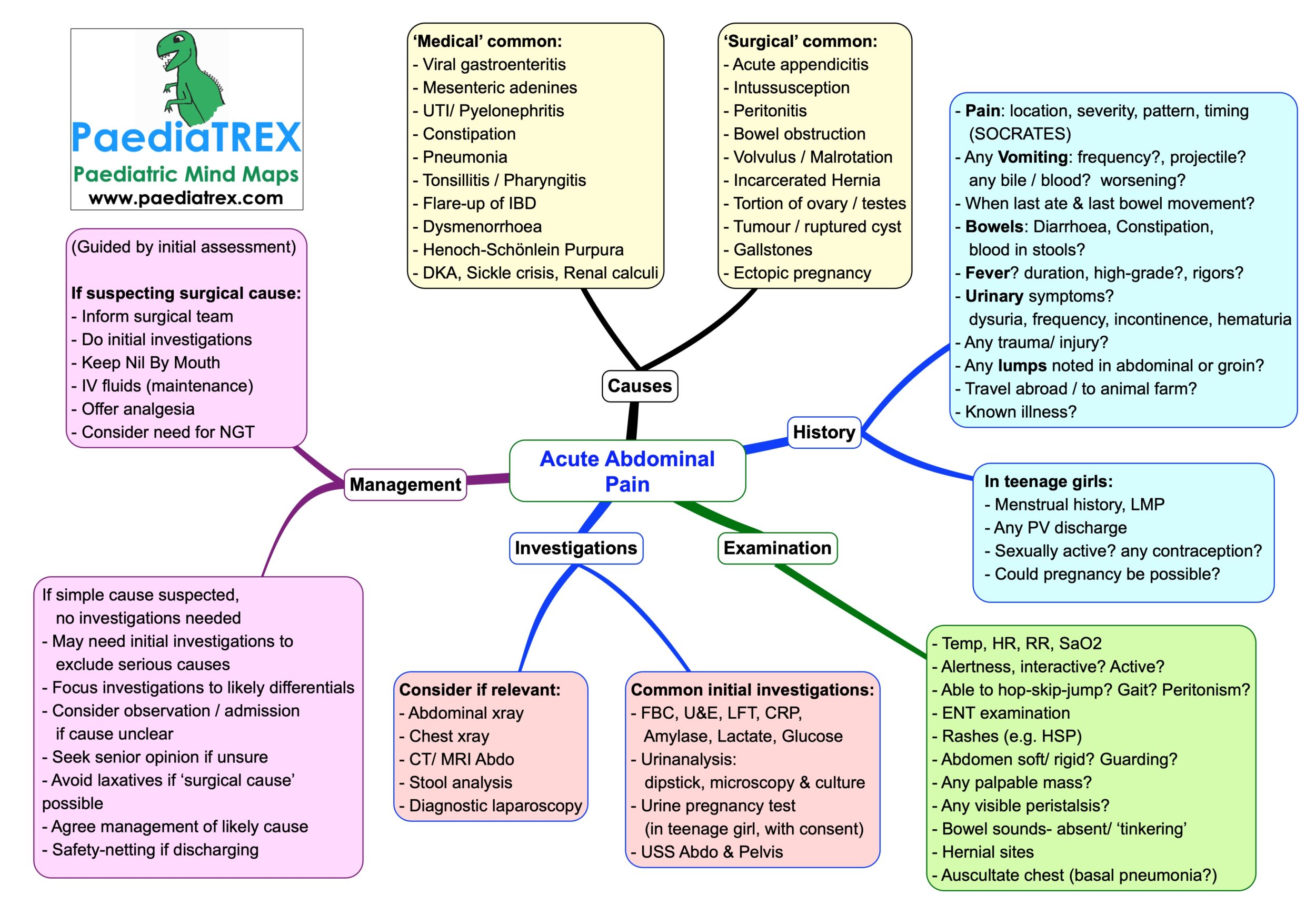
Acute Abdominal Pain
‘Medical’ common causes:
– Viral gastroenteritis
– Mesenteric adenines
– UTI/ Pyelonephritis
– Constipation
– Pneumonia
– Tonsillitis / Pharyngitis
– Flare-up of IBD
– Dysmenorrhoea
– Henoch-Schönlein Purpura
– DKA, Sickle crisis, Renal calculi
‘Surgical’ common causes:
– Acute appendicitis
– Intussusception
– Peritonitis
– Bowel obstruction
– Volvulus / Malrotation
– Incarcerated Hernia
– Tortion of ovary / testes
– Tumour / ruptured cyst
– Gallstones
– Ectopic pregnancy
History:
– Pain: location, severity, pattern, timing
(SOCRATES)
– Any Vomiting: frequency? projectile?
any bile / blood? worsening?
– When last ate & last bowel movement?
– Bowels: Diarrhoea, Constipation, blood in stools?
– Fever? duration, high-grade?, rigors?
– Urinary symptoms?
dysuria, frequency, incontinence, hematuria
– Any trauma/ injury?
– Any lumps noted in abdominal or groin?
– Travel abroad / to animal farm?
– Known illness?
In teenage girls:
– Menstrual history, LMP
– Any PV discharge
– Sexually active? any contraception?
– Could pregnancy be possible?
Examination:
– Temp, HR, RR, SaO2
– Alertness, interactive? Active?
– Able to hop-skip-jump? Gait? Peritonism?
– ENT examination
– Rashes (e.g. HSP)
– Abdomen soft/ rigid? Guarding?
– Any palpable mass?
– Any visible peristalsis?
– Bowel sounds- absent/ ‘tinkering’
– Hernial sites
– Auscultate chest (basal pneumonia?)
Common initial investigations:
– FBC, U&E, LFT, CRP, Amylase, Lactate, Glucose
– Urinanalysis: dipstick, microscopy & culture
– Urine pregnancy test (in teenage girl, with consent)
– USS Abdo & Pelvis
Consider if relevant:
– Abdominal xray
– Chest xray
– CT/ MRI Abdo
– Stool analysis
– Diagnostic laparoscopy
Management: (Guided by initial assessment)
If suspecting surgical cause:
– Inform surgical team
– Do initial investigations
– Keep Nil By Mouth
– IV fluids (maintenance)
– Offer analgesia
– Consider need for NGT
No investigation needed if simple cause suspected.
– May need initial investigations to exclude serious causes
– Focus investigations to likely differentials
– Consider observation / admission if cause is unclear
– Seek senior opinion if unsure
– Avoid laxatives if ‘surgical cause’ possible
– Agree management of likely cause
– Safety-netting if discharging
Leung AKC; Sigalet DL Acute abdominal pain in children. American Family Physician. June 1, 2003. Vol.67,Iss11; pg.2321
Hijaz NM, Friesen CA. Managing acute abdominal pain in pediatric patients: current perspectives. Pediatric Health Med Ther. 2017;8:83–91.