
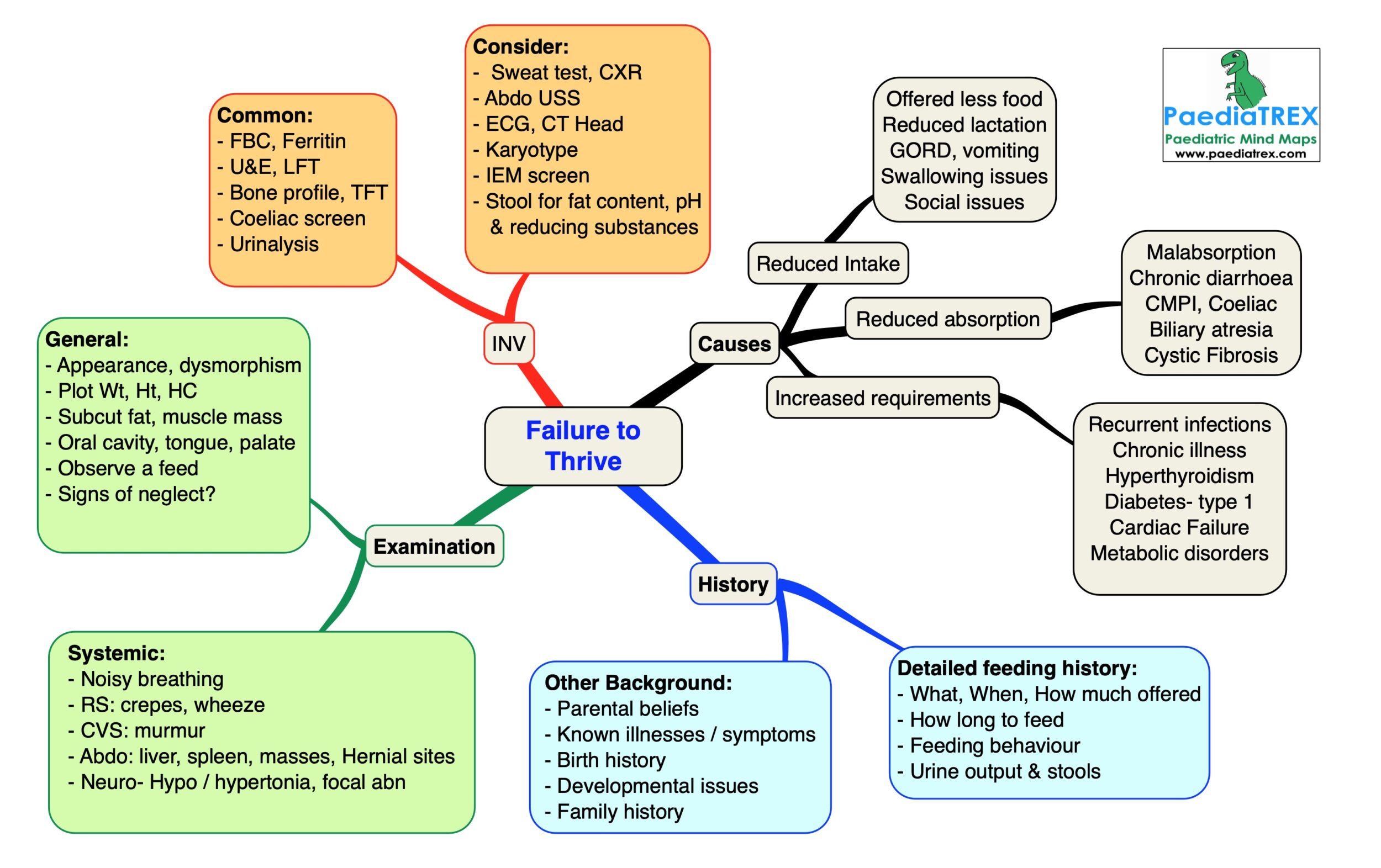
Failure to thrive (Faltering Growth)
History:
Detailed feeding history:
– What, When, How much offered
– How long to feed
– Feeding behaviour
– Urine output & stools
Other Background:
– Parental beliefs
– Known illnesses / symptoms
– Birth history
– Developmental issues
– Family history
Examination:
General:
– Appearance, dysmorphism
– Plot Wt, Ht, HC
– Subcut fat, muscle mass
– Oral cavity, tongue, palate
– Observe a feed
– Signs of neglect?
Systemic:
– Noisy breathing
– RS: crepes, wheeze
– CVS: murmur
– Abdo: liver, spleen, masses, Hernial sites
– Neuro- Hypo / hypertonia, focal abn
Causes:
Reduced intake:
– Offered less food
– Reduced lactation
– GORD, vomiting
– Swallowing issues
– Social issues
Reduced absorption:
– Malabsorption
– Chronic diarrhoea
– CMPI, Coeliac
– Biliary atresia
– Cystic Fibrosis
Increased requirements:
– Recurrent infections
– Chronic illness
– Hyperthyroidism
– Diabetes- type 1
– Cardiac Failure
– Metabolic disorders
Investigations:
Common:
– FBC, Ferritin
– U&E, LFT
– Bone profile, TFT
– Coeliac screen
– Urinalysis
Consider if relevant:
– Sweat test, CXR
– Abdo USS
– ECG, CT Head
– Karyotype
– IEM screen
– Stool for fat content, pH
& reducing substances
NICE guideline. Faltering growth: recognition and management of faltering growth in children (2017)
Shields B, Wacogne I, Wright CM; Weight faltering and failure to thrive in infancy and early childhood. BMJ. 2012 Sep 25345:e5931.
Kerzner B, et al; A practical approach to classifying and managing feeding difficulties. Pediatrics. 2015 Feb135(2):344-53.