
Kawasaki disease
Have a low index of suspicion in a young child with fever plus other features described below, due to the risk of coronary vessel complication.
Treat as Kawasaki disease with IVIG if
Fever for 5 days + any 4 of
– Eyes: bilat conjunctivitis, no discharge
– Mouth: Red-Cracked lips / Strawberry tongue
– Neck: Cervical LN >1.5cm, often unilateral
– Skin: diffuse maculopapular or urticarial rash
– Hands / feet: redness/ oedema/ peeling
Consider differentials of KD:
– Scarlet fever (Group A Streptococcus)
– Infectious mononucleosis (EBV)
– Stevens-Johnson syndrome
– Allergic / Drug reactions
– Toxic shock syndrome
Assessment:
– Common vasculitis resulting in coronary artery aneurysm
– Consider diagnosis if fever + rash with above criteria suggesting multi-systemic inflammation
– Self-resolves in 12- 14 days
– Consider the diagnosis early
Investigations suggested:
Bloods:
– FBC, raised platelets after 7 days
– U&E, CRP, LFT, ESR
– Blood culture
ECHO:
– Immediately as baseline
– Repeat in 6 weeks
Urinanalysis
ECG
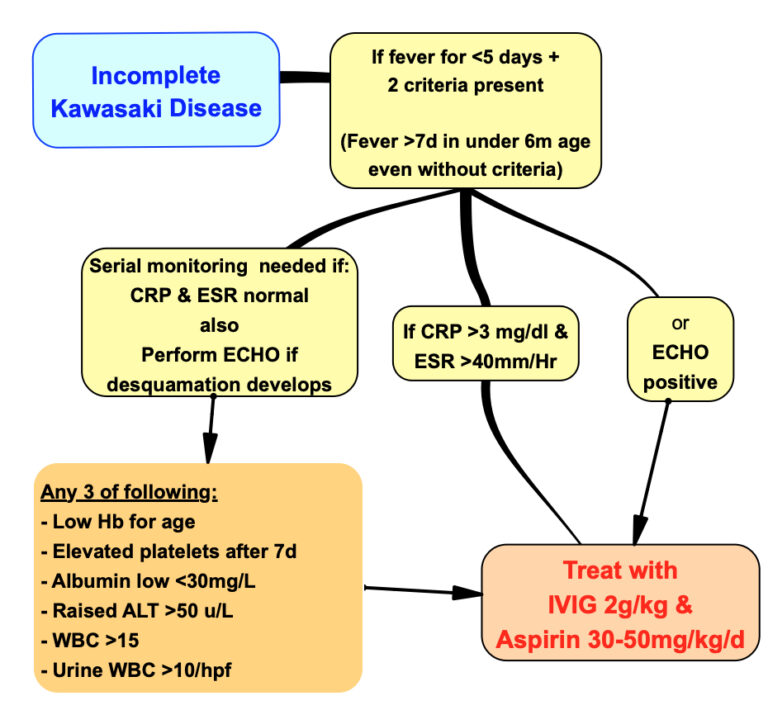
Diagnosis requires at least 5 days of fever and any 4 of recognition features; however
► KD can nowbe diagnosed with 4days of fever when 4 features are present (particularly if erythema and oedema of hands / feet).
► KD should be considered even if fever resolves after 7days without treatment.
► KD should also be considered in:
– Infants under 6 months of age with prolonged fever and irritability.
– Infants with prolonged fever and aseptic meningitis.
– Infants or children with prolonged fever plus unexplained lymphadenitis, retrotonsillar collection or shock.
KD can be excluded if CRP, ESR and platelet count are normal after 7 days of fever.
ESR becomes uninterpretable after administering IVIG.
Echocardiography is not a diagnostic test for KD, so do not delay treatment if ECHO is unavailable or is normal.
Coronary artery abnormality is not usually detectable until after 7 days of illness.
Coronary artery internal diameter z-score greater than or equal to 2.5 is highly specific for KD.
If KD suspected, do ECHO within 1–2 weeks, and then 4–6 weeks after initial treatment; if both normal then no further imaging needed.
What is long term management of KD?
Management includes prevention of thrombosis and minimising progression of coronary artery aneurysms.
Serial echocardiography and cardiology follow-up are recommended to monitor for changes in cardiac function and/or coronary vessels.
The AHA updated guideline provides risk-stratified recommendations and frequency of cardiology assessment required.
Live vaccines should be delayed until at least 11 months after IVIG, as antibodies in IVIG may reduce the effectiveness of these vaccines.
Reference:
Phuong LK, Chen KY, Burgner DP, et al. What paediatricians need to know about the updated 2017 American Heart Association Kawasaki disease guideline. Archives of Disease in Childhood 2020;105:10-12.